Oxaliplatin-based therapy: strategies to prevent or minimize neurotoxicity
WCRJ 2014; 1 (2): e232
Topic: Pharmacogenomics, Translational research
Category: Review
Abstract
BACKBONE: Oxaliplatin is an anticancer drug used to treat some different neoplasms: lung, colorectal, ovarian, breast, head/neck, and genitourinary. Moreover, patients treated with oxaliplatin more often discontinue therapy due to peripheral neuropathy and not to tumor progression. Patient benefit is potentially compromising. Several strategies are been investigated to prevent neurotoxicity.
CONTENT: In order to overcome this life-altering side effect, while taking advantage of the antineoplastic activities of the oxaliplatin, we detail recent findings of the , most common available strategies methods for prevention/minimize neurotoxicity. These include: a) variation of the standard scheduling; b) addition of various neurological drug to standard protocol; c) use of “natural” antioxidant agents.
CONCLUSIONS: Based on these actions, the oncologists will have a new issues with which to make treatment decisions for their patients to maximize benefit and minimize neurotoxicity. Based on this purpose, the clinician and pharmacists may join to evaluate advantages and limitation, in terms of costs and applicability, of the most appropriate strategies to incorporate routinely into clinical practice.
INTRODUCTION
Toxicity profile of Oxaliplatin is well documented and often this adverse reaction leads to the suspension of therapy and potentially compromises patient benefit. Primarily toxicities include severe peripheral neuropathy linked to acute and cumulative doses of Oxalipaltin 1. Current evidences have reported different polymorphisms associated to same adverse drug response 2. However, since the clinical expertise to interpret pharmacogenomics data is low, the clinical application of these genetic variants remains unclear, and controversial 3. In addition, emerging new evidences in nutrigenomics field, and new issues like stress and fatigue in cancer patients 4, suggesting an accurate evaluation of the diet during oxaliplatin therapy 5.
Several studies have suggested minimizing the neurotoxicity of oxaliplatin through the use of different compounds. These compounds include both natural substances and drugs. Specific examples include calcium and magnesium infusions, but they appear to reduce the effectiveness of chemotherapy, (moreover for someone calcium and magnesium do not prevent the neurotoxicity 6. Furthermore, Guilongtongluofang is promising to prevent oxaliplatin-inducedneurotoxicity in patients with colorectal cancer, but does not reduce the efficacy of oxaliplatin 7 , 8.Altun ZS et al 9 have suggested that also Acetyl-L-Carnitine (ALC) could be an agent against cytotoxicity induced by cisplatin without interfering to therapeutic index. Already, since the year 2000, Conklin KA had proposed the use of antioxidant molecules to minimize the adverse side effects of chemotherapy 10.
Pharmacological approaches include neurological drugs primarily as venlafaxine and Duloxetine 11, suitable for concomitant infusion with oxaliplatin.
The aim of this review is to provide information for the oncologist on the advantage and limitations, of the most common available strategies methods for prevention toxicity by improving the best scheduling approach to minimize cumulative toxicity. Perhaps, to this end, it might be possible to even consider a personalized diet 12.
METABOLIC FATE OF OXALIPLATIN AND PROPOSED MODEL OF TOXICITY
The cytotoxic lesion of platinating agents is primarily supposed to be the platinum intrastrand crosslink that forms on DNA, although treatment triggers a number of signal transduction pathways. Others proposed mechanism for oxaliplatin, including immunogenic signals for tumour cells before apoptosis, triggering Interferon gamma production and interaction with dendritic cells via Toll Like receptor4 resulting in death of cancer cells 13.
All platinating drugs get aquated when entering into a cell, losing chloride or oxalate ions. This positively charged molecule is then capable of interacting with nucleophilic molecules within the cell, as well DNA, RNA, and proteins. When the platinating agents binding to DNA ribbon the N7 atoms of the guanosine and adenosine nucleotide bases. Purine bases can form four different types of lesions on DNA: monoadducts, intrastrand crosslinks, and interstrand crosslinks and DNA-Crosslink 14. The result is the contortion of the DNA. Than those formed from cisplatin or carboplatin, oxaliplatin adducts are bulkier and more hydrophobic. These features lead to different effects, which is likely contributing to the differences in toxicity 15. The amount of DNA cross-links in neurons at a specified cumulative dose was significantly correlated with the level of neurotoxicity 16. Patient trials of platinum agents have revealed that the seriousness of neurotoxicity is commonly cisplatin > oxaliplatin >> carboplatin. Cisplatin and oxaliplatin suffer hydrolysis to a greater extent than carboplatin, which can bring to the difference in the associated neurotoxicity severity patterns.
Oxaliplatin-based regimens
Despite a modest activity as a single agent, oxaliplatin exert significant activity in combination with other drugs especially used in combination with Fluoropirimidines 17. Treatment in conjunction with 5-FU/LV (FOLFOX) have shown improved survival in the adjuvant setting among Stage III patients compared to 5-FU/ LV and 5-FU/irinotecan treatments 18. Importantly, the incidence of low neurotoxicity associated with 5-FU, is increased with the addition of Oxaliplatin 19. The Food and Drug Administration (FDA) noted that over 70% of the patients receiving oxaliplatin are involved by some degree of peripheral neuropathy 20, including ototoxicity and dysphonic syndrome 21. Notably, neurotoxicity, and not tumor progression, is often the cause of treatment discontinuation. Despite these adverse life-altering side effects, Oxaliplatin therapy have a key role for the treatment choice in a large setting of cancer patients (pancreas, colon-rectum, lung, lymphoma, etc); including in the so called frail patients (i.e. elderly and HIV-positive patients) 22 , 23 , 24 for whom the efficacy and especially the toxicity profile are important aspects 25 , 26.
STRATEGIES APPROACH FOR PREVENTION/MINIMIZE OF CUMULATIVE NEUROTOXICITY
Several approaches have been optimized to prevent or minimize the cumulative neurotoxicity associated with Oxaliplatin therapy. These include interrupting and reintroducing oxaliplatin administration, lengthening the duration of infusion, various pharmacologic agents (i.e., calcium/magnesium, glutathione, etc.) and antioxidant “natural medicines”.
Stopping and reintroducing oxaliplatin
When significant neuropathy develops during treatment, it is reasonable to discontinue theoxaliplatin and to switch to an oxaliplatin-free chemotherapy regimen allowing as much recovery as possible before reintroducing oxaliplatin. Many authors suggest that interspersing an oxaliplatin-free “maintenance” regimen is a reasonable maneuver to prevent/minimize the development of neuropathy in responding patients who have received oxaliplatin-based therapy for 3-4 months with no clinically significant neuropathy. Data from the OPTIMOX-1 (maintenance with 5-FU/LV), OPTIMOX-2 (complete stop and restart of FOLFOX after 6 months) 27 and CONcePT trials (alternating schedule of 8 weeks mFOLFOX followed by 8 weeks of 5-FU/LV plus bevacizumab), suggest that this strategy decreases the risk of severe neuropathy without compromising antitumor efficacy 28. However, continuous treatment with oxaliplatin is also an option in patients undergoing palliative chemotherapy for metastatic colorectal cancer, particularly in a responding patient with aggressive and/or bulky disease who is well tolerating the chemotherapy. In this setting, the chemotherapy-free intervals have the potential to worsen outcomes and are not recommended.
Lengthened infusion duration
Benefits from prolonging the duration of the infusion appears to be limited in preventing the acute neuropathy. The dose-limiting, cumulative neurotoxicity is not influenced by the duration of infusion or fractionation and is only dependent on the cumulative dose administered. Lengthening the duration of the oxaliplatin infusion from two to six hours has been evaluated in a randomized trial, in which 64 patients receiving adjuvant chemotherapy for colorectal or gastric carcinoma have been randomly assigned to six- or two-hour infusions of oxaliplatin 29 , 30. The overall percentage of patients with sensory neurotoxicity has not been significantly decreased with the six-hour infusion (84% vs. 93% with the two-hour infusion), although there has been a significant decrease in the number of treatment cycles with grade 2 or greater neurotoxicity (6% vs. 19%).
The utility of this approach is limited by the logistical issues associated with a prolonged infusion, combined with the lack of effect on cumulative neurotoxicity.
Pharmacologic approaches
Several pharmacologic agents have shown properties to diminish the incidence and the severity of neurotoxicity either in small randomized trials or uncontrolled studies. Although initial results have been promising for these agents, appropriately randomized trials are required to confirm the neuro-protective effect of an intervention and to rule out any interference with antitumor activity before these pharmacologic approaches can be widely adopted.
A multitude of agents are suitable for concomitant infusions with oxaliplatin; these include, calcium and magnesium 31, Velafaxine 32, glutamine 33, neurotropin 34 and the Japanese traditional herbal formula Goshajinkigan (Gosha-Jinki-Gan) 35, and others (Table 1).
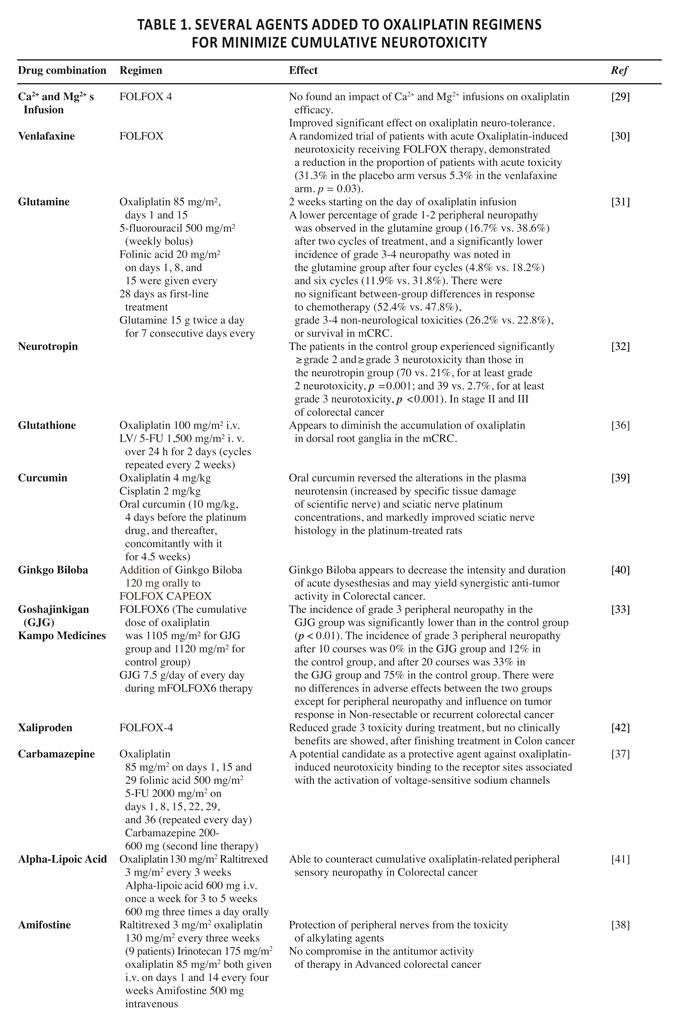
Table 1. Several agents added to oxaliplatin regimens for minimize cumulative neurotoxicity.
Benefits fromCalcium and magnesium infusions have been demonstrated by placebo-controlled phase III trials in patients receiving oxaliplatin for metastatic colorectal cancer (the CONcePT trial) and in the adjuvant setting (the N04C7 trial 36 ) in patients with advanced disease 37. However, a planned interim analysis of the first 180 patients enrolled in the CONcePT trial has found a significantly lower response rate in patients treated with Ca/Mg compared to the control group 38.
It is reasonable that the lower response rates in patients with metastatic colorectal cancer who received IV Ca/Mg in conjunction with oxaliplatin have not been established in subsequent preliminary reports detailing independent blinded central review of the response data from the CONcePT trial, or in a preliminary report of patients with metastatic disease who have been enrolled on the randomized French NEUROXO study.
In the CAIRO2 trial comparing capecitabine,oxaliplatin, andbevacizumab with or without cetuximab 39, the prophylactic use of Ca/Mg has been performed in 551 patients before and after the oxaliplatin infusion at least during the first treatment cycle with 369 (67%) receiving prophylaxis for all six oxaliplatin infusions while 181 have not received Ca/Mg during the first cycle. There has been a trend toward a lower incidence of all-grade late neurotoxicity with Ca/Mg (30% vs. 39%, p = 0.07), but with comparable incidence of grade > 2 neurotoxicity. While there has been significantly less all-grade acute neurotoxicity with Ca/Mg (81 vs. 91%), differences in the rates of ≥ grade 2 acute neurotoxicity have not been statistically significant (27% vs. 34%, p = 0.06).
In summary, these data suggest that supplemental Ca/Mg infusions may reduce some forms ofneurotoxicity. However, there is still no strong data from an adequately powered prospective randomized study in advanced disease on which to base the assessment of the real value of the Ca/Mg infusions and their relationship to progression-free or overall survival.
Potential benefit fromVenlafaxine has been suggested in a small placebo-controlled randomized trial conducted in 48 patients who developed distressing oxaliplatin-induced acute neurotoxicity 40. Patients have been randomly assigned to venlafaxine 50 mg one hour prior to the oxaliplatin infusion followed by 37.5 mg twice daily from days 2 to 11 or placebo. The proportion of patients experiencing full relief of acute neurotoxicity during subsequent cycles of therapy has been significantly higher in the venlafaxine group (31% vs. 5%). Furthermore, at three months post-treatment, at a time when no patient remained on oxaliplatin therapy, a significantly higher number of patients in the venlafaxine arm had no neurotoxicity (39% vs. 6%), and significantly fewer have had grade 3 neurotoxicity (0 vs. 33%).
Wang WS et al 41 have demonstrated that a lower percentage of grade 1-2 peripheral neuropathy has been obtained by glutamineaddiction compared to standard therapy (16.7% vs. 38.6%) after two cycles of treatment, and a significantly lower incidence of grade 3-4 neuropathy after four (4.8% versus 18.2%) and six cycles (11.9% vs. 31.8%).
Attempts to improve the tolerability of oxaliplatin have been done through the combined use of Neurotropin. Benefits from this association have been shown by trials enrolled patients with grade 2-3 neurotoxicity randomly divided into two groups, one of which received neurotropin treatment: significantly results have been reported in the neurotropin group 42. Other drugs, including Glutathione 43, carbamazepine 44, Amifostine 45, have been also successfully tested.
It is reported that several “natural medicines” like as curcumin 46, ginkgo biloba 47, alpha-lipoic acid 48 and the Kampo medicine, Goshajinkigan 49, has been considered effective neuro-protective agents, without adverse effects.
Taken together and given the lack of confirmatory evidence that these pharmacologic agents interfere with antitumor efficacy, it is reasonable to consider them, at least in patients being treated with oxaliplatin. Until further information is available, we would not pursue this approach in the adjuvant setting. Accrual to a confirmatory randomized, placebo-controlled trial in patients receiving adjuvant therapy for colon cancer has been completed by the North Central Cancer Treatment Group (NCCTC, NCT00316914), which should settle the question of whether this therapy is worthwhile and safe in the adjuvant setting.
While these data seem promising, confirmation in larger trials is needed. Noticeable, the potential pitfalls of relying upon phase II studies to guide practice, can be illustrated by the experience with xaliproden, a neurotrophic agent that showed promise in small phase II studies. A phase III trial has been conducted in which 649 patients have been randomly assigned to xaliproden or placebo in conjunction with oxaliplatin-based chemotherapy. In a preliminary report presented in 2006, there has been a lower incidence of grade 3 sensory neuropathy with xaliproden (17% vs. 11% with placebo). However, the overall incidence of neurotoxicity was the same (73% on both arms), there was no increase in the total cumulative dose of oxaliplatin, or in the time patients could remain on treatment, or the percentage of patients with complete recovery after treatment with oxaliplatin (49% vs. 47%). Thus, there appeared to be no clinically meaningful benefit from the use of xaliproden 50.
CONCLUSIONS AND FUTURE OUTLOOK
Strategies previously described allowing physicians to improve the efficacy of cancer therapy. On the other hand, the clinical utility of the described strategies in Oxaliplatin based-therapy is in part limited by the evidence that natural remedies improve clinical outcomes is still an open question. The cost-effectiveness of these procedures is unknown.
Results from several strategic approaches optimized for management of oxaliplatin-induced neuropathy seem promising, but confirmation in larger trials is still needed.
Many of natural protective substances against toxicity of oxaliplatin are antioxidants. There are some of these that have been studied by several authors such as calcium and magnesium or Guilongtongluofang. An italian working group has demonstrated that the repetitive administration of antioxidants silibinin (the principal component of the silymarin complex) and a-tocopherol reduced oxaliplatin-dependent pain 51.
Over the next few years, it is fundamental that pharmaceutical companies develop extensive trials on the standardization strategies suitable for routine clinical application in Oxaliplatin therapy.
CONCLUSIONS
With the increasing number of novelvalidated Oxaliplatin based schedules, oncologists willhave new means to make treatment decisions, as well as correlation between nutrition and cancer 52 , 53, and may eventually be personalized on the patients in order to minimize toxicity 54.
Based on these purposes, the clinician and the pharmacists may join together to estimate advantages and restriction, in terms of costs and applicability, of the most suitable strategies to scheduling in oxaliplatin based therapy.
AKNOWLEDGEMENTS: the authors are grateful to Dr. O. Barletta from the “Italian Association of Pharmacogenomics and Molecular Diagnostics” for the invaluable bibliography research, and Mrs Paola Favetta for her expert assistant in the preparation and correction of the manuscript.
REFERENCES
- Kidwell KM, Yothers G, Ganz PA, Land SR, Ko CY, Cecchini RS, Kopec JA, Wolmark N. Long-term neurotoxicity effects of oxaliplatin added to fluorouracil and leucovorin as adjuvant therapy for colon cancer: results from National Surgical Adjuvant Breast and Bowel Project trials C-07 and LTS-01. Cancer 2012; 118: 5614-5622. (back)
- Di Francia R, Siesto RS, Valente D, Del Buono A, Pugliese S, Cecere S, Cavaliere C, Nasti G, Facchini G, Berretta M. Current strategies to minimize toxicity of oxaliplatin: selection of pharmacogenomic panel tests. Anticancer Drugs 2013; 24: 1069-1078. (back)
- Di Francia R, Pugliese S, Del Buono A, Berretta M. What health professions in oncology needs to know about pharmacogenomics?. World Cancer Res J 2014; 1: e90. (back)
- Giacalone A, Spina M, Berretta M, Tirelli U. Two types of fatigue in cancer patients. Br J Cancer 2012; 106: 424; author reply 5. (back)
- Cappellani A, Cavallaro A, Di Vita M, Zanghi A, Piccolo G, Lo Menzo E, Cavallaro V, Malaguarnera M, Giaquinta A, Veroux M, Cimino L, Berretta M. Diet and pancreatic cancer: many questions with few certainties. Eur Rev Med Pharmacol Sci 2012; 16: 192-206. (back)
- Loprinzi CL, Qin R, Dakhil SR, Fehrenbacher L, Flynn KA, Atherton P, Seisler D, Qamar R, Lewis GC, Grothey A. Phase III randomized, placebo-controlled, double-blind study of intravenous calcium and magnesium to prevent oxaliplatin-induced sensory neurotoxicity (N08CB/Alliance). J Clin Oncol 2014; 32: 997-1005. (back)
- Liu Y, Zhu G, Han L, Liu J, Ma T, Yu H. Clinical study on the prevention of oxaliplatin-induced neurotoxicity with guilongtongluofang: results of a randomized, double-blind, placebo-controlled trial. Evid Based Complement Alternat Med 2013; 2013: 541217. (back)
- Kono T, Hata T, Morita S, Munemoto Y, Matsui T, Kojima H, Takemoto H, Fukunaga M, Nagata N, Shimada M, Sakamoto J, Mishima H. Goshajinkigan oxaliplatin neurotoxicity evaluation (GONE): a phase 2, multicenter, randomized, doubleblind, placebocontrolled trial of goshajinkigan to prevent oxaliplatininduced neuropathy. Cancer Chemother Pharmacol 2013; 72: 1283-1290. (back)
- Altun ZS, Gunes D, Aktas S, Erbayraktar Z, Olgun N. Protective effects of acetyl-L-carnitine on cisplatin cytotoxicity and oxidative stress in neuroblastoma. Neurochem Res 2010; 35: 437-443. (back)
- Conklin KA. Dietary antioxidants during cancer chemotherapy: impact on chemotherapeutic effectiveness and development of side effects. Nutr Cancer 2000; 37: 1-18. (back)
- Piccolo J, Kolesar JM. Prevention and treatment of chemotherapy-induced peripheral neuropathy. Am J Health Syst Pharm 2014; 71: 19-25. (back)
- Harvie M. Nutritional supplements and cancer: potential benefits and proven harms. Am Soc Clin Oncol Educ Book 2014; 34: e478-86. (back)
- Martins I, Kepp O, Schlemmer F, Adjemian S, Tailler M, Shen S, Michaud M, Menger L, Gdoura A, Tajeddine N, Tesniere A, Zitvogel L, Kroemer G. Restoration of the immunogenicity of cisplatin-induced cancer cell death by endoplasmic reticulum stress. Oncogene 2011; 30: 1147-1158. (back)
- Rabik CA, Dolan ME. Molecular mechanisms of resistance and toxicity associated with platinating agents. Cancer Treat Rev 2007; 33: 9-23. (back)
- Hah SS, Stivers KM, de Vere White RW, Henderson PT. Kinetics of carboplatin-DNA binding in genomic DNA and bladder cancer cells as determined by accelerator mass spectrometry. Chem Res Toxicol 2006; 19: 622-626. (back)
- Dzagnidze A, Katsarava Z, Makhalova J, Liedert B, Yoon MS, Kaube H, Limmroth V, Thomale J. Repair capacity for platinum-DNA adducts determines the severity of cisplatin-induced peripheral neuropathy. J Neurosci 2007; 27: 9451-9457. (back)
- Berretta M, Lleshi A, Di Benedetto F, Bearz A, Spina M, Tirelli U. Oxaliplatin and capecitabine (Xelox) in association with highly active antiretroviral therapy in advanced hepatocarcinoma HIV/HCV-infected patients. Ann Oncol 2006; 17: 1176-1177. (back)
- Goldberg RM, Sargent DJ, Morton RF, Fuchs CS, Ramanathan RK, Williamson SK, Findlay BP, Pitot HC, Alberts SR. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol 2004; 22: 23-30. (back)
- Cecchin E, D’Andrea M, Lonardi S, Zanusso C, Pella N, Errante D, De Mattia E, Polesel J, Innocenti F, Toffoli G. A prospective validation pharmacogenomic study in the adjuvant setting of colorectal cancer patients treated with the 5-fluorouracil/leucovorin/oxaliplatin (FOLFOX4) regimen. Pharmacogenomics J 2012; 13: 403-409. (back)
- Ibrahim A, Hirschfeld S, Cohen MH, Griebel DJ, Williams GA, Pazdur R. FDA drug approval summaries: oxaliplatin. Oncologist 2004; 9: 8-12. (back)
- Berretta M, Taibi R, Bearz A, La Mura N, Berretta S, Tirelli U, Frustaci S. Dysphonia as an unusual toxic event of oxaliplatin-based chemotherapy. J Chemother 2004; 16: 595-598. (back)
- Berretta M, Bearz A, Frustaci S, Talamini R, Lombardi D, Fratino L, Lleshi A, Bonanno S, Spartà D, Palmucci S, Berretta S, Tirelli U. FOLFOX2 in the treatment of advanced colorectal cancer: a comparison between elderly and middle aged patients. J Chemother 2008; 20: 503-508. (back)
- Berretta M, Lleshi A, Cappellani A, Bearz A, Spina M, Talamini R, Cacopardo B, Nunnari G, Montesarchio V, Izzi I, Lanzafame M, Nasti G, Basile F, Berretta S, Fisichella R, Schiantarelli C C, Garlassi E, Ridolfo A, Guella L, Tirelli U. Oxaliplatin based chemotherapy and concomitant highly active antiretroviral therapy in the treatment of 24 patients with colorectal cancer and HIV infection. Curr HIV Res 2010; 8: 218-222. (back)
- Berretta M, Di Benedetto F, Bearz A, Simonelli C, Martellotta F, Del Ben C, Berretta S, Spina M, Tirelli U. FOLFOX-4 regimen with concomitant highly active antiretroviral therapy in metastatic colorectal cancer HIV-infected patients: a report of five cases and review of the literature. Cancer Invest 2008; 26: 610-614. (back)
- Berretta M, Lleshi A, Cappellani A, Bearz A, Spina M, Talamini R, Cacopardo B, Nunnari G, Montesarchio V, Izzi I, Lanzafame M, Nasti G, Basile F, Berretta S, Fisichella R, Schiantarelli C C, Garlassi E, Ridolfo A, Guella L, Tirelli U. Oxaliplatin based chemotherapy and concomitant highly active antiretroviral therapy in the treatment of 24 patients with colorectal cancer and HIV infection. Curr HIV Res 2010; 8: 218-222. (back)
- Pumo V. Di Mari A, Rametta Giuliano S, Bordonaro S, Iacono M, Roccaro S, Iemmolo S, Lanteri E, Romano F, Tralongo P. Life after lung cancer: survivorship research and behavioral intervention are needed. WCRJ 2014; 1(1): e100. (back)
- Chibaudel B, Tournigand C, Bonnetain F, Maindrault-Goebel F, Lledo G, André T, Larsen AK, Bengrine-Lefevre L, Louvet C, de Gramont A. Platinum-sensitivity in metastatic colorectal cancer: towards a definition. Eur Rev Cancer 2013; 49: 3813-3820. (back)
- Grothey A, Sargent DJ. New lessons from “old” chemotherapy in colorectal cancer. J Clin Oncol 2008; 26: 4532-4534. (back)
- Petrioli R, Pascucci A, Francini E, Marsili S, Sciandivasci A, Tassi R, Civitelli S, Tanzini G, Lorenzi M, Francini G. Neurotoxicity of FOLFOX-4 as adjuvant treatment for patients with colon and gastric cancer: a randomized study of two different schedules of oxaliplatin. Cancer Chemother Pharmacol 2008; 61: 105-111. (back)
- Argyriou AA, Cavaletti G, Briani C, Velasco R, Bruna J, Campagnolo M, Alberti P, Bergamo F, Cortinovis D, Cazzaniga M, Santos C, Papadimitriou K, Kalofonos HP. Clinical pattern and associations of oxaliplatin acute neurotoxicity: a prospective study in 170 patients with colorectal cancer. Cancer 2013; 119: 438-444. (back)
- Gamelin L, Capitain O, Morel A, Dumont A, Traore S, Anne le B, Gilles S, Boisdron-Celle M, Gamelin E. Predictive factors of oxaliplatin neurotoxicity: the involvement of the oxalate outcome pathway. Clin Cancer Res 2007; 13: 6359-6368. (back)
- Durand JP, Deplanque G, Montheil V, Gornet JM, Scotte F, Mir O, Cessot A, Coriat R, Raymond E, Mitry E, Herait P, Yataghene Y, Goldwasser F. Efficacy of venlafaxine for the prevention and relief of oxaliplatin-induced acute neurotoxicity: results of EFFOX, a randomized, double-blind, placebo-controlled phase III trial. Ann Oncol 2012; 23: 200-205. (back)
- Wang WS, Lin JK, Lin TC, Chen WS, Jiang JK, Wang HS, Chiou TJ, Liu JH, Yen CC, Chen PM. Oral glutamine is effective for preventing oxaliplatin-induced neuropathy in colorectal cancer patients. Oncologist 2007; 12: 312-319. (back)
- Zhang RX, Lu ZH, Wan DS, Wu XJ, Ding PR, Kong LH, Pan ZZ, Chen G. Neuroprotective effect of neurotropin on chronic oxaliplatin-induced neurotoxicity in stage II and stage III colorectal cancer patients: results from a prospective, randomised, single-centre, pilot clinical trial. Int J Colorectal Dis 2012; 27: 1645-1650. (back)
- Nishioka M, Shimada M, Kurita N, Iwata T, Morimoto S, Yoshikawa K, Higashijima J, Miyatani T, Kono T. The Kampo medicine, Goshajinkigan, prevents neuropathy in patients treated by FOLFOX regimen. Int J Clin Oncol 2011; 16: 322-327. (back)
- Grothey A, Sargent DJ. New lessons from “old” chemotherapy in colorectal cancer. J Clin Oncol 2008; 26: 4532-4534. (back)
- Gamelin L, Capitain O, Morel A, Dumont A, Traore S, Anne le B, Gilles S, Boisdron-Celle M, Gamelin E. Predictive factors of oxaliplatin neurotoxicity: the involvement of the oxalate outcome pathway. Clin Cancer Res 2007; 13: 6359-6368. (back)
- Kurniali PC, Luo LG, Weitberg AB. Role of calcium/magnesium infusion in oxaliplatin-based chemotherapy for colorectal cancer patients. Oncology (Williston Park) 2010; 24: 289-292. (back)
- Knijn N, Tol J, Koopman M, Werter MJ, Imholz AL, Valster FA, Mol L, Vincent AD, Teerenstra S, Punt CJ. The effect of prophylactic calcium and magnesium infusions on the incidence of neurotoxicity and clinical outcome of oxaliplatin-based systemic treatment in advanced colorectal cancer patients. Eur Rev Cancer 2011; 47: 369-734. (back)
- Durand JP, Deplanque G, Montheil V, Gornet JM, Scotte F, Mir O, Cessot A, Coriat R, Raymond E, Mitry E, Herait P, Yataghene Y, Goldwasser F. Efficacy of venlafaxine for the prevention and relief of oxaliplatin-induced acute neurotoxicity: results of EFFOX, a randomized, double-blind, placebo-controlled phase III trial. Ann Oncol 2012; 23: 200-205. (back)
- Wang WS, Lin JK, Lin TC, Chen WS, Jiang JK, Wang HS, Chiou TJ, Liu JH, Yen CC, Chen PM. Oral glutamine is effective for preventing oxaliplatin-induced neuropathy in colorectal cancer patients. Oncologist 2007; 12: 312-319. (back)
- Zhang RX, Lu ZH, Wan DS, Wu XJ, Ding PR, Kong LH, Pan ZZ, Chen G. Neuroprotective effect of neurotropin on chronic oxaliplatin-induced neurotoxicity in stage II and stage III colorectal cancer patients: results from a prospective, randomised, single-centre, pilot clinical trial. Int J Colorectal Dis 2012; 27: 1645-1650. (back)
- Cascinu S, Catalano V, Cordella L, Labianca R, Giordani P, Baldelli AM, Beretta GD, Ubiali E, Catalano G. Neuroprotective effect of reduced glutathione on oxaliplatin-based chemotherapy in advanced colorectal cancer: a randomized, double-blind, placebo-controlled trial. J Clin Oncol 2002; 20: 3478-3483. (back)
- von Delius S, Eckel F, Wagenpfeil S, Mayr M, Stock K, Kullmann F, Obermeier F, Erdmann J, Schmelz R, Quasthoff S, Adelsberger H, Bredenkamp R, Schmid RM, Lersch C. Carbamazepine for prevention of oxaliplatin-related neurotoxicity in patients with advanced colorectal cancer: final results of a randomised, controlled, multicenter phase II study. Invest New Drugs 2007; 25: 173-180. (back)
- Penz M, Kornek GV, Raderer M, Ulrich-Pur H, Fiebiger W, Scheithauer W. Subcutaneous administration of amifostine: a promising therapeutic option in patients with oxaliplatin-related peripheral sensitive neuropathy. Ann Oncol 2001; 12: 421-422. (back)
- Al Moundhri MS, Al-Salam S, Al Mahrouqee A, Beegam S, Ali BH. The effect of curcumin on oxaliplatin and cisplatin neurotoxicity in rats: some behavioral, biochemical, and histopathological studies. J Med Toxicol 2013; 9: 25-33. (back)
- Mahdy HM, Tadros MG, Mohamed MR, Karim AM, Khalifa AE. The effect of Ginkgo biloba extract on 3-nitropropionic acid-induced neurotoxicity in rats. Neurochem Int 2011; 59: 770-778. (back)
- Gedlicka C, Scheithauer W, Schull B, Kornek GV. Effective treatment of oxaliplatin-induced cumulative polyneuropathy with alpha-lipoic acid. J Clin Oncol 2002; 20: 3359-3361. (back)
- Nishioka M, Shimada M, Kurita N, et al. The Kampo medicine, Goshajinkigan, prevents neuropathy in patients treated by FOLFOX regimen. Int J Clin Oncol 2011; 16: 322-327. (back)
- Susman E. Xaliproden lessens oxaliplatin-mediated neuropathy. Lancet Oncol 2006; 7: 288. (back)
- Di Cesare Mannelli L, Zanardelli M, Failli P, Ghelardini C. Oxaliplatin-induced neuropathy: oxidative stress as pathological mechanism. Protective effect of silibinin. J Pain 2012; 13: 276-284. (back)
- Berretta M, Lleshi A, Fisichella R, Berretta S, Basile F, Li Volti G, Bolognese A, Biondi A, De Paoli P, Tirelli U, Cappellani A. The role of nutrition in the development of esophageal cancer: what do we know? Front Biosci 2012; 4: 351-357. (back)
- Berretta M, Cappellani A, Lleshi A, Di Vita M, Lo Menzo E, Bearz A, Galvano F, Spina M, Malaguarnera M, Tirelli U, Berretta S. The role of diet in gastric cancer: still an open question. Front Biosci 2012; 17: 1640-1647. (back)
- Berretta M. DFR, Tirelli U. The new oncologic challenges in the 3RD millennium. WCRJ 2014; 1(1): e133. (back)
To cite this article
Oxaliplatin-based therapy: strategies to prevent or minimize neurotoxicity
WCRJ 2014; 1 (2): e232
Publication History
Published online: 01 Jul 2014

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.